









 12 / 38
12 / 38

New Mexico Dental Journal, Spring 2015
12
Five Common Implant Complications
W
hat an exciting time in the
era of dentistry in which
we practice, where dental
implants have become a successful and
predictable option for restoring missing
teeth. In fact, systematic reviews have
shown that success rates that started
at 77.6% in the early days of dental
implants are now documented at an
average of 96.8% (Pjetursson and
coworkers 2014).
Everyone who places and/or restores
implants in their practice has seen the
marvelous benefits to both the patients
as well as to their practices. Predictable,
stable, long-term results are what we all
desire. However, at some point, each of us
will be faced with difficult complications
relating to dental implants. In this article
I will discuss five common problems
seen when treating patients with dental
implants. I will also offer solutions
regarding how to address those problems
when they arise. Obviously, there are
many other potential complications that
can arise. However, for the purpose of
this article, I have chosen what, in my
opinion, are five of the most common
dental implant complications I encounter
in my practice. All the images used were
taken at my private office and none have
been photoshopped (except for figure 6
where two images were superimposed for
illustrative purposes). A more in-depth
analysis of each of these complications
may be addressed at a later date.
1. Improper Angulation
2. I nadequa t e r e s t or a t i ve spac e/
Improper implant depth
3. Aesthetic failures due to material
selection/wrong abutment selection/
poor emergency profile
4. Hardware failure - broken screws,
broken abutments, broken implants
5. Implant failure - failure secondary to
cementation technique, due to lack of
hygiene, overloading.
1
Improper Angulation
Improper angulation of the implant
is perhaps one of the most common
problems I encounter as a prosthodon-
tist. Sadly, it is one of the most easily
preventable. When an implant is placed
such that the platform is too close to the
adjacent teeth, too far labially, or too far
lingually, it becomes difficult to impress
and restore. Implants placed at the
wrong angle may not be fully surrounded
by bone, which can lead to failure (See
Figures 2 and 13). It also can lead to
dramatic esthetic failures (See Figure 1)
that can be very costly (in time, money,
and confidence) to repair. So who is at
fault and how do we prevent this?
I would submit that the surgeon and
restorative dentist share the blame
equally most of the time. While at a
recent meeting of Dental Laboratory
Technicians, I asked the question,
“What is the most frustrating problem
you have to deal with?” Their answer
was a resounding “
lack of planning
.” It
is unreasonable for restorative dentists
to expect prefect placement of implants
when little to no planning was done
nor when a
quality
surgical guide was
not made
and used
. To surgeons I
recommend that you do not place the
implant without a quality guide (See
Figure 13). To dentists I recommend
that you do not let your surgeon place
Dr. Norby is a specialist in Prosthodontics and owns and operates
a private practice limited to Prosthodontics in Albuquerque, NM.
He is also a Certified Laboratory Technician in the specialty of
Ceramics and Complete Dentures.
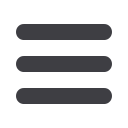
Figure 1
—Implant platform exposed on recently placed implant. The implant was placed
immediately following extraction without a surgical guide. The poor esthetic outcome
is exacerbated by the high lip line.
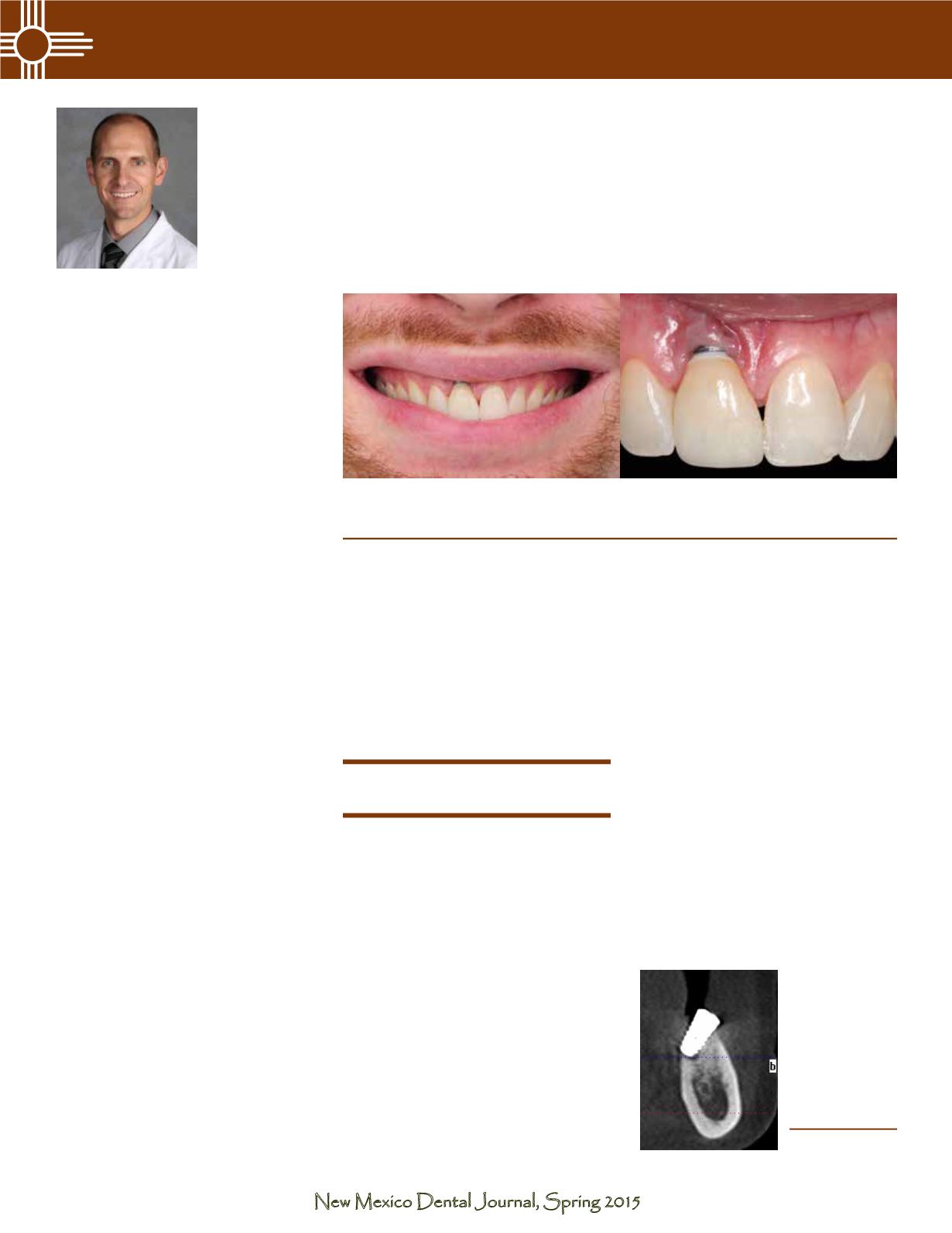
Figure 2
—CBCT
image showing
a 6 week ol d
implant placed
at a severe angle
outside of the
lingual plate in
the #19 position.
By Darren C. Norby, DMD, CDT