









 17 / 38
17 / 38

17
nmdental.org
disrupt even a healthy system. Here are
some key points to remember:
• Torque implant s to approved
torque values
• Torque abutment screws to manu-
facturer torque specifications
• Remember to calibrate your torque
wrenches periodically.
• Evaluate cantilever forces and avoid
excessive cantilevers
• Always adjust to ideal occlusion
(which many times is only light
contact on average masticatory
systems)
• Cover abutment screw with cotton
and a temporary filling to facilitate
retrieval if ever necessary
5
Implant failure. Failure
due to cementation
technique, lack of
hygiene, poor placement,
or overloading.
Although overall implant success is
now reported as very high, implant fail-
ures still occur, which is frustrating for
both the patient and dental team. More
and more recent research is strongly
suggesting that excess cement is a signifi-
cant factor in long-term failure of dental
implants. Recent data indicate that
biological complications are significantly
more frequent in cemented restorations
compared to screw retained restorations
(Wittneben and Millen 2014). Great care
must be exercised when cementing an
implant crown to avoid lodging cement
(See Figure 12) around the implant.
Consequently, it may be impossible to
remove the cement without surgical
intervention.
I recent ly had a pat ient pre sent
complaining of a persistent pain
around a new (less than 6 months)
screw-retained implant crown on #4.
Clinically she presented with a fistula
on the palatal aspect of #4 implant. The
patient reported that she had already
been prescribed antibiotics two times
and even had the crown remade once
without any resolution to the problem.
After radiographic examination revealed
no positive findings, I removed the new
implant crown and carefully ran my
probe around the platform of the implant
and dislodged a small piece of excess
cement (Figure 11). So even though the
crown had been cemented onto the
abutment outside the mouth and then
screwed down, meticulous cleaning of
excess cement was not performed, nor
was the crown-abutment interface well-
polished. The cement flash separated
from the crown and became an irritant
that was impossible for the patient to
remove, leading to the gingival abscess.
After cleaning any remaining excess
cement and adding a high polish with
porcelain polishing burs, the crown was
torqued back into place. The patient
returned after 10 days stating that the
pain was gone for the first time since the
crown was delivered. The gingival lesion
was healed as well.
Overloading of dental implants also can
lead to implant failure. If an implant is
moved while osteoblasts are growing
around the threads, osseointegration
cannot take place fully. After integra-
tion, implants can still disintegrate
under large, irregular forces. To avoid
this, some general guidelines can be
applied. Primarily, don’t use narrow
diameter implants in the posterior or to
fill large edentulous spaces. Addition-
ally, splinting multiple implants can
help spread the load to any given implant
when a force is applied. This concept is
well-illustrated in many modern studies
using a Finite Elemental Analysis to
compare forces to peri-implant bone
on single implants vs. splinted implants
when lateral forces are applied.
Fig 11
—Abscess caused by excess cement around the platform of screwretained crown
on implant #4. 10 days later the lesion almost fully healed.
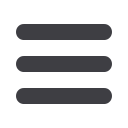
Fig 12
—Example of excess cement on
another cement retained crown.
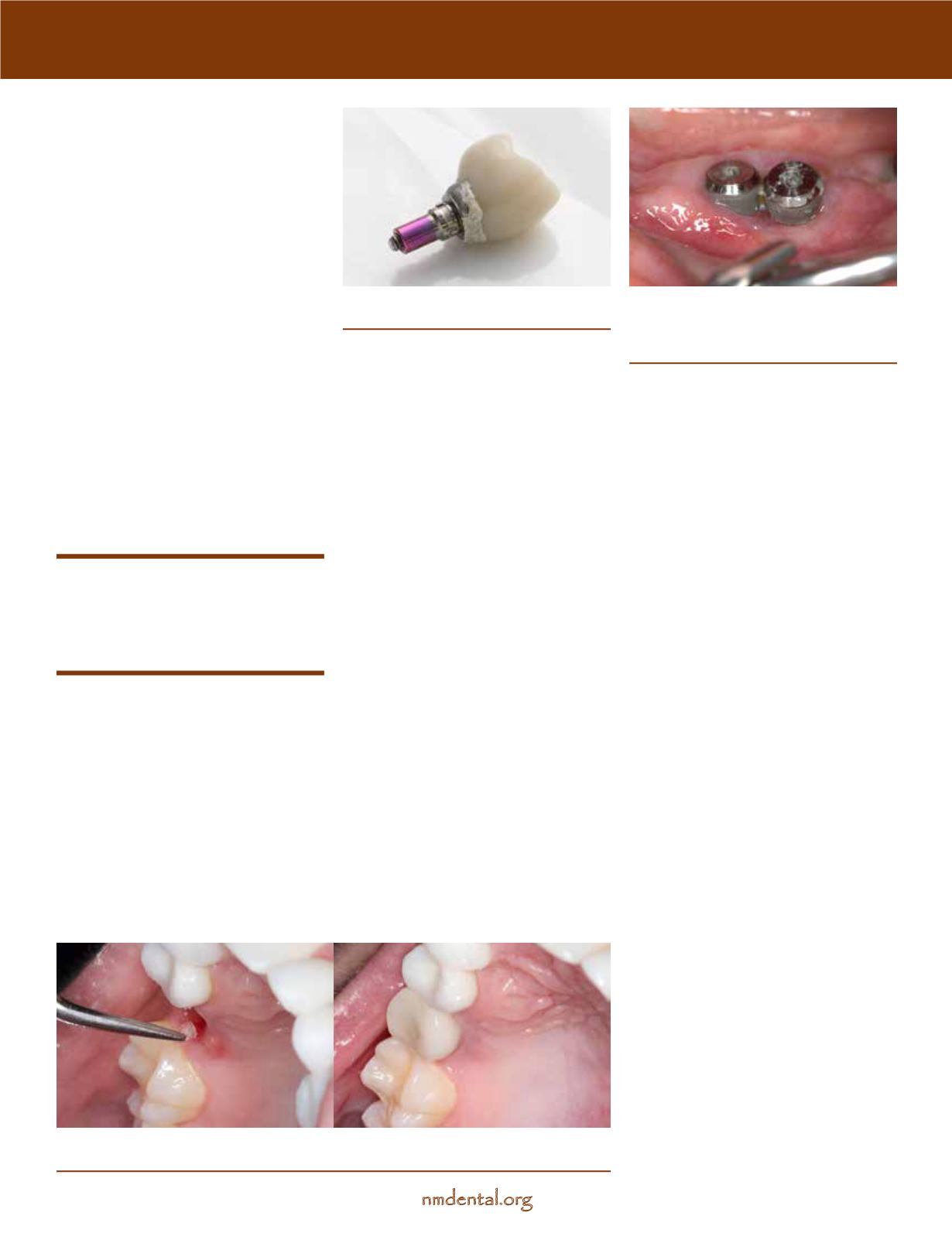
Fig 13
—Two failing implants placed too
close to each other 6 weeks post-place-
ment. Note the absence of bone on the
buccal and interproximal aspect.
continues