








 19 / 40
19 / 40

The average daily requirement for vita-
min B
12
is 1-2micrograms. Naturally oc-
curring vitamin B
12
can only be manu-
factured by bacteria in animal products.
The main source of dietary vitamin B
12
is shellfish, liver, fish, crab, fortified
soy products, fortified cereals, cheese
and eggs.
4
vitamin B
12
deficiency causes
megaloblastic (pernicious) anemia, dam-
age to the white mater of the brain and
spinal cord and peripheral neuropathy.
Pernicious anemia onset is at a young
age and slowly over time with glossodyn-
ia and one of the signs and symptoms of
the disease. Neurologic manifestations
can be summarized as weakness and
hyporeflexia and loss of vibratory sensa-
tion in the hands and feet with a stock-
ing-glove distribution. Some patients
may be irritable and mildly depressed.
Glossodynia and atrophic glossitis com-
prise the myriad of signs and symptoms
of B
12
deficiency. Clinical manifesta-
tions of atrophic glossitis are character-
ized by smooth, shiny appearance of the
tongue from the loss of filiform papillae.
The etiology is believed to be the effect
on the rapidly dividing epithelial cells of
the mouth and gastrointestinal tract.
3
Laboratory diagnosis is confirmed with
CBC, vitamin B
12
(cobalamin) and B
6
(folate) levels and/or Shilling test (for
suspected intrinsic factor deficiency re-
lated pernicious anemia).
The hallmark of treatment of glossodyn-
ia secondary to vitamin B
12
deficiency is
supplemental vitamin B
12
. Regardless of
the etiology of vitamin B
12
deficiency,
high-dose oral
Supplementation of crystalline B
12
is
1,000 to 2,000mcg daily for 2 weeks,
followed by 1,000mcg daily for main-
tenance is currently recommended.
Nasal gel preparation and oral drops
are also available which are absorbed
directly into the blood through oral or
nasal mucous membranes and there-
fore bypass the GI absorption route.
B
12
(cyanocobalamin injectable form)
1000micriograms may be given IM 1mg
1 to 4 times per week for several weeks
until resolutions of symptoms and then
a maintenance regimen of 1mg IM every
4 weeks. Effective B
12
therapy will cor-
rect blood counts (pernicious anemia)
in 2 months and neurologic symptoms,
glossitis and glossodynia in 6 months.
6
17
nmdental.org
References
1
Julia S. Lehman,* Alison J. Bruce,
†
and Roy S. Rogers III.
†
“Atrophic Glossitis From Vitamin B
12
Deficiency:
A Case Misdiagnosed as Burning Mouth Disorder.
J Periodontology
December 2006; 77(12):2090-2092.
2
Larry Johnson MD PhD. Vitamin B
12
(cobalamins)
Merck Manual
, October 14
3
Hélder Antônio Rebelo Pontes, DDS, MSc, PhD; Nicolau Conte Neto, DDS; Karen Bechara Ferreira, DDS; Felipe Paiva Fonseca;
Gizelle Monteiro Vallinoto; Flávia Sirotheau Corrêa Pontes, DDS, MSc, PhD; Décio dos Santos Pinto Jr, DDS, MSc, PhD.
Oral Manifestations of Vitamin B
12
Deficiency: A Case Report.
JCDA
September 2009, Vol. 75, No. 7
4
www.healthconsious.com Top 10 Foods highest in Vitamin B
12
(Cobalamin)
5
National institute of Dental and Craniofacial research. Burning mouth syndrome. www.nidcr.gov
6
Sally P. Stabler, M.D. Vitamin B
12
Deficiency.
N Engl J Med
2013;368:149-60.
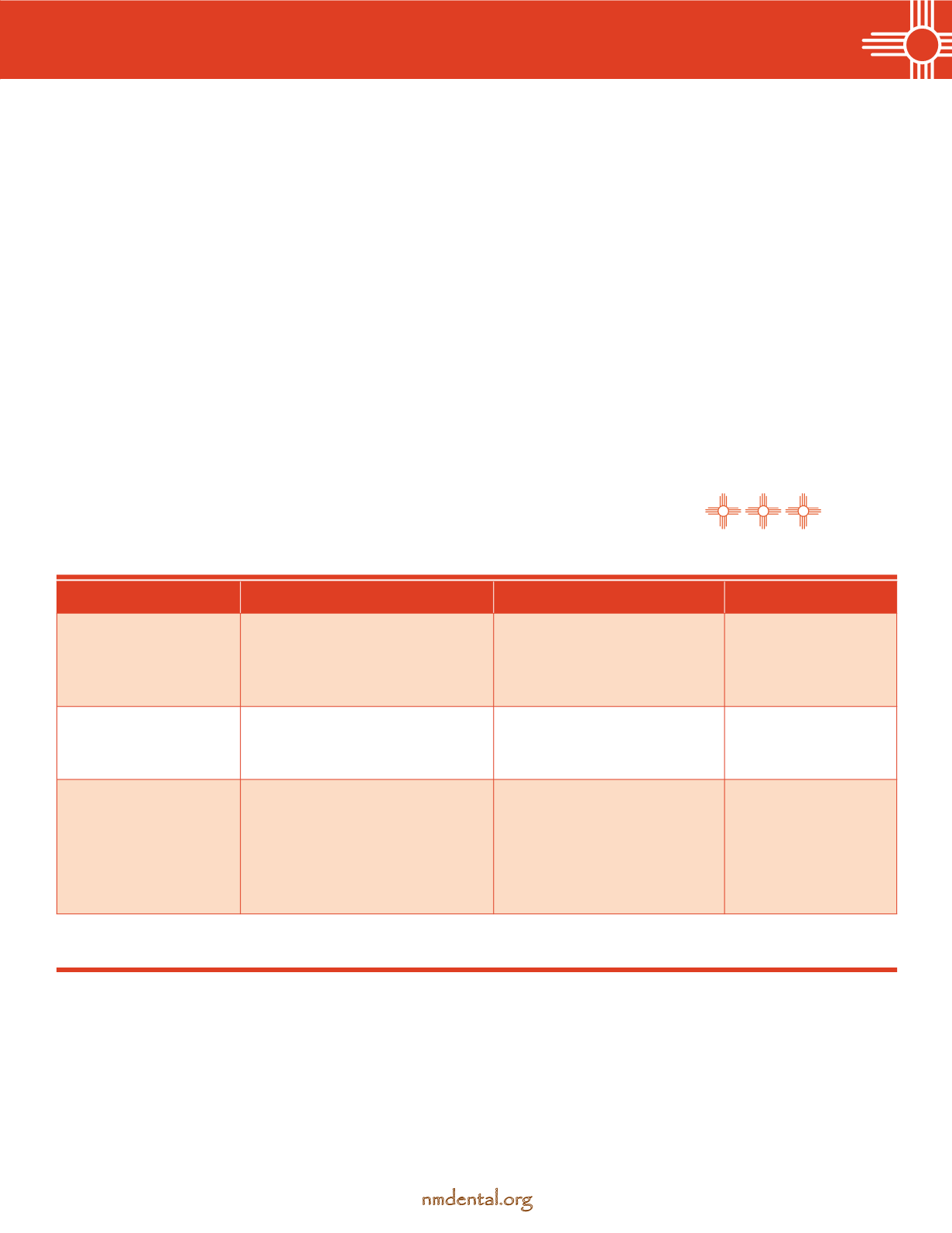
Condition
Clinical presentation
Studies
Treatment
Vitamin B
12
deficiency
Beefy, red, smooth dorsal tongue.
Glossodynia. Atrophic glossitis.
Serum B
12
. Note that serum B
12
in the low normal range
(<100 pg per milliliter)
may have symptoms.
6
Vitamin B
12
PO, injections, and/
or oral-nasal drops.
Oral candidiasis
White coating of the dorsal tongue
which generally scrapes off with a
tongue depressor.
Potassium hydroxide prep
of a tongue scraping
Systemic or topical
antifungal therapy.
Burning Mouth
Disorder/syndrome
Generalized oral mucosal pain that
is scalding, burning or tingling,
in the absence of identifiable oral
mucosal lesions. The tongue is
most frequently affected.
5
No specific test. Rule out
medical condition that may be
the root cause, i.e. Sjögren’s
syndrome, meds that cause
xerostomia, GERD, hormone
deficiency.
5
Palliative therapy and
avoid triggering agents,
i.e. tobacco, alcohol,
citrus, spicy food.
Differential diagnosis